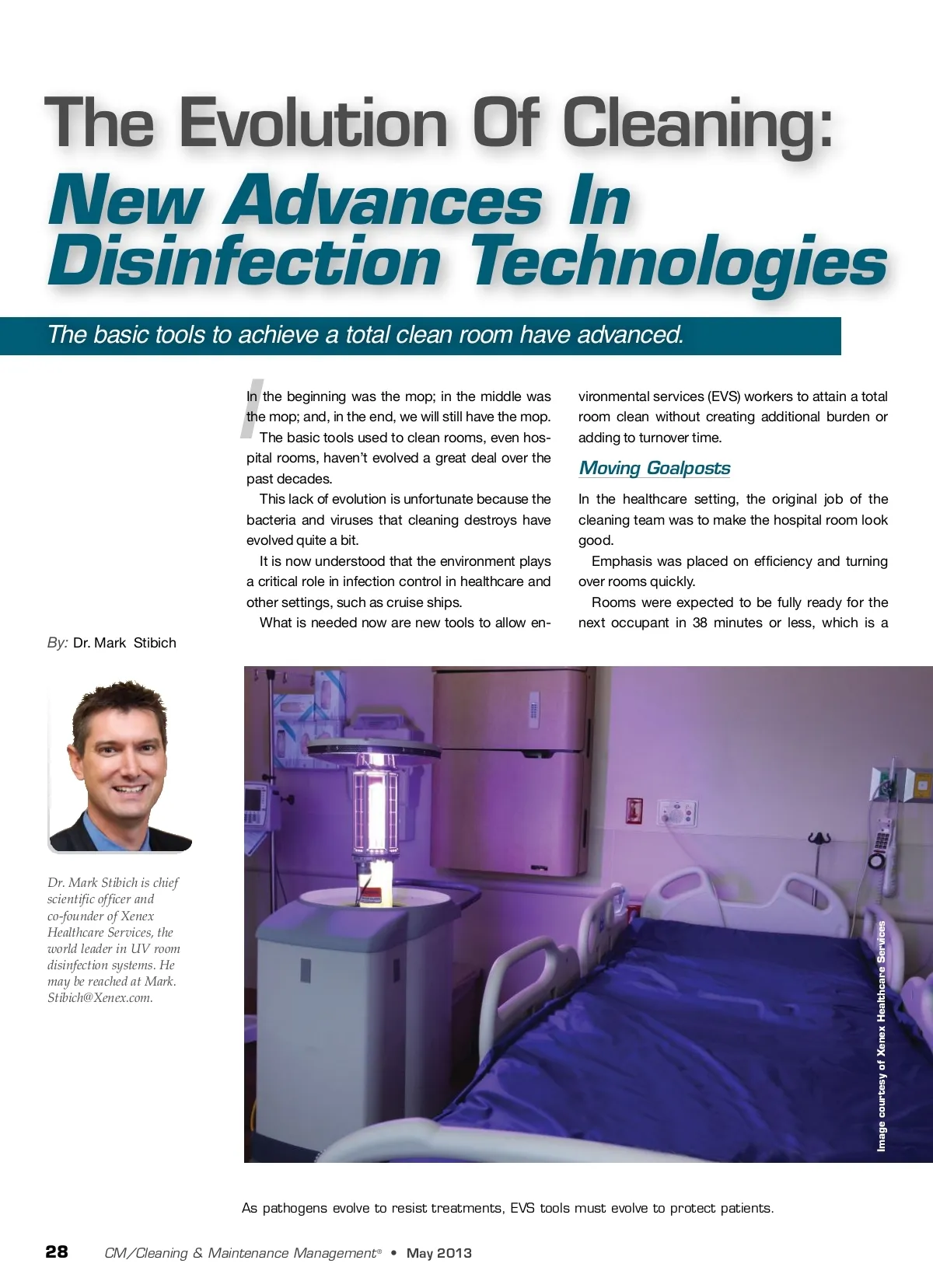
challenging feat by anyone’s standards. As researchers learn more and more about how the environment can contribute to infections, that goal is changing. At recent conferences, the term “patho-gen-free room” has been suggested as the new goal of the environmental services team. This, of course, is a necessary and noble goal: to make certain that the environment cannot harm the patient. Of course, it is also a challenging goal: to make certain that no infectious bacteria or viruses are left behind in a room. Unfortunately, one thing was forgotten when this goal was created; the cleaning team wasn’t given any more time or any new tools to accomplish the goal of the “patho-gen-free room.” The same efficiency standards are in place, but the stakes have changed. The resources are the same, but the goal-posts have been moved far away. is needed are new methods and tools for ac-complishing that goal. ships and other markets in the near future. Real-world Expectations In order for any of these systems to protect patients and reduce infection rates, it must integrate into real-world situations without excessive costs or disruption of patient flow. In a busy hospital, a disinfecting system that is too slow, complex to use or is cost-ly will not be used often enough to have a meaningful impact on hospital-acquired in-fection (HAI) rates. No-touch disinfection systems do not op-erate themselves. Someone has to move the devices around the hospital and operate them. Who that person is will be a very impor-tant consideration in choosing a no-touch disinfection system. Some of the no-touch disinfection systems can be operated by a housekeeper and others require a more in-depth technical training. Look for a system that has been designed specifically for use by the EVS team — easy to transport and easy to use. No-touch Disinfection No-touch disinfection is a category that is rapidly emerging in the hospital environmen-tal cleaning space and will likely expand into other areas in the near future. The category is so new that there are a wide variety of names for it: Room disin-fection, automatic disinfection, total room cleaning and more. Hospitals seem to be settling on the term “no-touch disinfection” to describe a num-ber of different technologies that automate the disinfection of rooms and equipment. There are essentially three main technolo-gies used for no-touch disinfection: hydro-gen peroxide vapor, mercury-vapor lamps and pulse xenon lamps. The first uses a familiar disinfectant — hy-drogen peroxide — and applies it in a vapor or mist throughout the room. The next two use different methods to pro-duce ultraviolet light in the germicidal spec-trum. Mercury vapor lamps produce germicidal ultraviolet in a narrow spectrum around 253.7 nanometers, while pulsed xenon produces ultraviolet that covers the entire UV germi-cidal spectrum (from 200-280 nanometers). Each technology, based on the published literature, takes a different amount of time to accomplish the goal of disinfection of bacte-rial spores — for example, the most difficult organism typically found in hospital rooms, C. diff . with hydrogen peroxide vapor taking at least 2.5 hours per room, mercury ultra-violet taking at least 50 minutes and pulsed xenon taking at least 15 minutes total. All of the technologies work, but each has a different profile in terms of the total disinfection and the total time required for disinfection. Recently, the Association for Profession-als in Infection Control (APIC) came out with new guidelines for the control of C. diff . These guidelines include references to “no-touch disinfection” systems and exam-ine the role of these new technologies in in-fection prevention in the hospital. These guidelines show the acceptability of “no-touch disinfection” in hospitals. It should be anticipated that these technol-ogies will be coming to nursing homes, cruise Room Cleaning: A Matter Of Life And Death The average person who cleans a hospital room today must be familiar with an alpha-bet soup of bacteria: MRSA, VRE, CRE, C. diff , MDRO, GNR, NDM-1, etc. For some of these organisms, there is es-sentially no treatment for the infection they cause. CRE, for example, has been described as a “nightmare bacteria” by the U.S. Centers for Disease Control and Prevention (CDC). To make matters worse, these organisms can also be resistant to the average disinfec-tant, forcing the use of bleach, which dam-ages surfaces and can create a harmful en-vironment for personnel. “Housekeepers” are rapidly becoming disinfection experts. Room cleaning has truly become a matter of life and death. Acute care hospitals are leading the charge to create safer environments. Environmental service directors sit on the infection control committee and are seen as an essential component of patient safety. Recent changes in reimbursement now link these infections directly to payments to the hospital by Medicare, Medicaid and pri-vate insurance. We know it is critically important to disin-fect every hospital room, every time — what Results Matter Most importantly, evaluate and consider the demonstrated impact the no-touch disin-fection systems are having on hospital in-fection rates. As these new technologies are deployed in real-world settings, the hospitals that de-ploy them may or may not report on the re-sulting infection rate changes. Devices that have been deployed for years without any reported infection rate impact may warrant cause for concern. Pulse xenon UV lamp systems already have demonstrated several in-hospital infec-tion rate reductions. For example, Cooley Dickinson Hospital was able to achieve a 53 percent drop in C. diff infections after implementing a pulse xe-non room disinfection system. The mop isn’t going anywhere (yet). But, the good news is that new technolo-gies (new tools) are here and allow EVS work-ers to attain a total room clean without creat-ing additional burden or adding to turnover time. As pathogens evolve to resist treatments, EVS tools must evolve to protect patients. We are seeing the start of that evolution today. CM www.cmmonline.com 29
CMM – Archives May 2013: 29